The clitoris is a fascinating and important part of female anatomy, often described as the pleasure center of the vulva. It is the only human organ whose sole known purpose is to provide sexual pleasure. Despite its significance, the clitoris has long been overlooked in both medical research and public discourse. Greater awareness and education are helping to change that, encouraging more open, informed conversations about female sexual health.
What Is the Clitoris?
The clitoris is a female sex organ that is highly sensitive and richly supplied with nerves. In humans, it is considered the most erogenous (sexually sensitive) part of the vulva and the primary anatomical source of female sexual pleasure. In fact, the human clitoris doesn’t play a direct role in reproduction - its only known function is to contribute to sexual arousal and orgasm. Because of this, it’s often said that the clitoris exists solely for pleasure.
Biologically, the clitoris is homologous to the penis in males. This means that during embryonic development, the clitoris and the penis originate from the same tissue (the genital tubercle) and share a similar structure in terms of erectile tissue and nerves. However, unlike the penis, the clitoris is not involved in urination or sperm delivery - it’s purely a pleasure organ. The visible tip of the clitoris may be small, but as we’ll see, the organ is much more extensive internally than it appears from the outside.
Location and External Anatomy
The clitoris is part of the vulva, which is the external genital area of people with female anatomy. Externally, the clitoris appears as a small nub of flesh located at the top of the vulva, where the inner labia (labia minora) meet. If you were looking at a diagram of a vulva, you’d find the clitoral glans (the visible part of the clitoris) just above the opening of the urethra (the tube you urinate from) and above the vaginal opening. In simple terms, it sits at the front, upper junction of the labia, usually under a fold of skin.
This fold of skin is known as the clitoral hood (or prepuce), and it partially or fully covers the clitoral glans. The hood is formed by the joining of the labia minora at the top of the vulva, and its purpose is to protect the sensitive glans. Just like individuals have different eye shapes or nose sizes, the clitoral hood can vary in size and how much of the glans it covers - in some people the glans is more exposed, while in others it’s mostly hidden beneath the hood. The hood can be gently retracted (moved aside) to expose the glans, similar to how a foreskin can retract from a penis (indeed, the clitoral hood is homologous to the foreskin).
The clitoral glans is the small, rounded visible tip. It’s often compared in size to a pea or a tiny button. On average, the glans might be about 4-5 millimeters across (roughly the size of a pea), but it can range from as little as ~2 mm to almost 1 cm in different individuals. This is perfectly normal - just like other body parts, clitoral size has natural variations. The glans itself is packed with nerve endings (about 8,000 of them, according to estimates) which makes it extremely sensitive to touch. In fact, the clitoral glans contains more nerve endings than any other part of the human vulva and about twice as many as the head of the penis, which is why it can produce very intense sensations of pleasure.
It’s important to note that what most people call the “clitoris” in everyday conversation - that little external nub - is actually just the glans of the clitoris. This is the tip of a much larger structure. To understand the full clitoris, we need to look beneath the surface at its internal anatomy.
Internal Anatomy and Structure
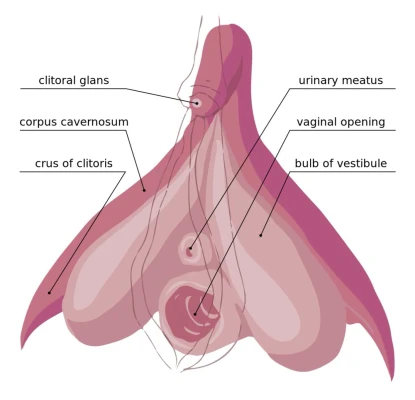

Although only the glans is visible externally, the majority of the clitoral structure lies inside the body. The clitoris can be imagined as a sort of upside-down wishbone or Y-shape that extends within the pelvis. Starting from the external glans, the clitoral organ extends inward as the body (or shaft) of the clitoris and then splits into two branches:
Clitoral Body (Shaft)
Just behind the glans (under the skin) is the clitoral body, sometimes called the shaft. This portion is made of erectile tissue (specifically two cylinders called the corpora cavernosa, similar to the erectile tissue in the penis). The body extends a short distance inward (anchored to the pubic bone by ligaments) before it branches. Think of the body as the stem of the wishbone before it forks.
Crura (Crus of the Clitoris)
The body of the clitoris splits into two elongated crura (Latin for "legs"). Each crus (singular) extends to the left and right, laterally along the pelvic bone. These crura are about 7-9 centimeters long in adults (2.5 to 3.5 inches) and form the “arms” of the wishbone-like structure. They stretch downward and backward from the clitoral body, flanking the vaginal canal and the urethra on either side. The crura are made of erectile tissue (continuations of the corpora cavernosa) that fill with blood during arousal.
Vestibular Bulbs
In addition to the crura, the clitoris includes two masses of erectile tissue called the vestibular bulbs (sometimes referred to as clitoral bulbs). These bulbs are on either side of the vaginal opening, kind of tucked under the labia minora. They are oval or bean-shaped masses of spongy tissue that also engorge with blood during sexual arousal. Each bulb is actually attached to a crus internally (they were historically considered separate, but functionally they are part of the clitoral complex). When a woman is aroused, the bulbs can swell to as much as double their resting size as they fill with blood.
All these parts - the glans, body, crura, and bulbs - are interconnected and meet at a central point known as the root of the clitoris (deep in the pelvis where the two “legs” join). The entire structure is sometimes called the clitoral complex or bulbo-clitoral organ, to emphasize that the clitoris is not just the external glans but a whole network of erectile tissue and nerves.
In terms of composition, the clitoris is made largely of erectile tissue (except the glans, which is a more dense nerve tissue cap). Erectile tissue is a spongy vascular tissue that can fill with blood and swell when aroused. This tissue in the clitoris is very similar to the tissue in a penis that causes an erection. So, during sexual arousal, the internal clitoris behaves a bit like a small internal “erection”: the crura and bulbs swell and stiffen with blood. This engorgement can cause the vulva (especially the labia minora and bulbs area) to puff up. Interestingly, as the vestibular bulbs swell, they actually hug the vaginal canal - this can add pleasurable pressure around the vagina and also help increase vaginal lubrication as part of the arousal response.
Because the internal clitoris surrounds the vagina (the bulbs sit on either side and the crura above), stimulation of the vagina often indirectly stimulates parts of the clitoris. We’ll talk more about this in the function section, especially in relation to the so-called G-spot.
To summarize the structure: the clitoris is much more than meets the eye. Externally you see the sensitive glans (often under its hood), but internally it stretches around the vaginal opening like a wishbone, composed of erectile “legs” and bulbs. This whole organ is richly supplied with nerves and blood vessels, making it highly sensitive and responsive during sexual activity.
Function: Sexual Pleasure and Arousal
The clitoris’s primary function is to generate sexual pleasure and to contribute to arousal and orgasm. In evolutionary or biological terms, the clitoris doesn’t have a reproductive job (unlike, say, the ovaries or uterus) - it exists to make sex feel good. This pleasure encourages sexual activity, which indirectly supports reproduction, but the clitoris itself isn’t needed to conceive a child. Essentially, nature provided the clitoris as a source of sexual enjoyment and excitement, which can strengthen bonding and make reproductive activities more likely.
What makes the clitoris so good at its job? Nerves! The clitoral glans alone is estimated to contain around 8,000 sensory nerve endings, which is one reason it’s extraordinarily sensitive. These nerves (including the dorsal nerve of the clitoris and branches of the pudendal nerve and cavernous nerves) link the clitoris to the spinal cord and brain, where sexual pleasure is ultimately processed. Stimulating the clitoris - whether through touch, pressure, vibration, or indirect stimulation - sends a cascade of pleasurable sensations to the brain. When sexual stimulation and arousal build up sufficiently, it can lead to a climax, or orgasm, which is a peak of intense pleasure accompanied by muscular contractions and release of tension.
For most people with vulvas, the clitoris is the key to reaching orgasm. It’s commonly reported that many women cannot orgasm from vaginal intercourse alone without clitoral stimulation. In fact, studies have shown that only a minority of women (~18% in one large survey) regularly climax from penetration alone, whereas a majority require direct clitoral stimulation or a combination of clitoral and vaginal stimulation to achieve orgasm. Often, direct stimulation of the clitoris (through touching the glans or rubbing the area) is what triggers orgasm, even if penetration is happening at the same time. One sexual health expert noted: “Direct stimulation to the glans clitoris or clitoral hood is usually needed for the final push to reach orgasm”. This is why activities like oral sex on the clitoris (cunnilingus) or manual stimulation (using fingers or sex toys on the clit) are very effective for many women to climax.
Indirect stimulation of the clitoris can also occur during vaginal intercourse. Because the internal parts of the clitoris (the bulbs and crura) surround the vaginal canal, penetration can press on or rub these internal clitoral structures through the vaginal walls. Some women find that a certain position or angle during intercourse increases clitoral pressure and leads to orgasm - this is essentially the internal clitoris being stimulated. The term G-spot is often used to describe a particularly sensitive area on the front wall of the vagina. Many researchers believe that what we call the G-spot is not a separate organ, but rather the sensitive internal part of the clitoral complex (the bulbs/crura) being stimulated through the vagina. As one urologist famously put it, “The vaginal wall is, in fact, the clitoris”, emphasizing that vaginal orgasm and clitoral orgasm are physiologically linked.
During sexual arousal, the clitoris undergoes changes: increased blood flow causes the internal parts to swell (as described earlier). The glans may also become more prominent as the surrounding tissue changes - in some cases, the glans can protrude more once aroused, while in other cases it might retract under the hood if it becomes very sensitive. The swelling of the bulbs and crura also contributes to what’s called the orgasmic platform - a buildup of muscular and tissue tension in the pelvis that occurs during arousal and is released during orgasm (the bulbs swelling add to the fullness in the vaginal opening area, and the pelvic floor muscles contract against them during climax). After orgasm (or after arousal subsides), the clitoris returns to its normal size as the blood flow reduces.
In summary, the function of the clitoris is to provide sexual pleasure and aid in orgasm. It’s the powerhouse of female sexual sensation. Even though it’s small in visible size, its extensive nerve network and erectile nature make it incredibly potent in its effects. A healthy, stimulated clitoris can produce intense pleasure, and understanding this organ can help individuals enhance their sexual experiences and satisfaction. Importantly, there's no “right” way to stimulate it - some may prefer gentle circling touches on the glans, others may like pressure through the hood, and some enjoy vibration. Knowing that the clitoris extends internally also helps in understanding that penetration can feel good largely because it’s stimulating the hidden parts of the clit.
Size, Appearance, and Variations
Just as people vary in height, hand size, or facial features, clitorises vary from person to person. Externally, the clitoral glans can range quite a bit in size. Typically it’s described as pea-sized (a few millimeters across), but medical studies have measured normal glans sizes anywhere from about 2 mm up to about 10 mm (roughly 1 cm). Most commonly, the diameter is around 5 mm (about 0.2 inches) in adult women. Some people might have a slightly more prominent glans that’s easily visible with the hood retracted, whereas others might have a very small glans that stays mostly under the hood. All of this is normal anatomy. The color of the glans and surrounding tissue can also vary - it is often pink or reddish, similar to the inner lips, but in people with more pigmented skin it may be brownish or darker. During arousal, increased blood flow might darken the color of the glans and labia, making them appear more flushed or swollen.
The clitoral hood can also differ in size and shape. Some hoods are short and don’t cover much of the glans at all, making the clitoris more exposed; others are longer and completely cover the glans unless manually pulled back. Neither is “better” - it’s just individual variation. A larger hood might require a bit more maneuvering to stimulate the glans directly, but it also provides protection, especially if the glans is very sensitive.
One interesting variation is how the clitoris responds during arousal. Because the glans itself has less erectile tissue (some sources consider it non-erectile or only minimally erectile), it doesn’t enlarge dramatically like a penis does. However, it may become slightly firmer or change position as the internal parts swell. In some individuals, arousal causes the clitoral glans to peek out from under the hood more (as blood engorges the area, the glans might protrude). In others, the hood might actually tighten over it (if the labia and surrounding tissues swell a lot, they can cover the glans more). Both responses are normal - some women notice their clit “popping out” when turned on, while others notice it seems to hide, and sensitivity can also fluctuate (often the glans becomes very sensitive after orgasm, sometimes to the point of being almost painful to touch until it calms down).
Internally, the overall size of the clitoral complex also varies. Research by Australian urologist Helen O’Connell and others showed that the combined length of the clitoris (from the glans, through the body, and down the crura) can be around 9-11 cm (3.5-4.3 inches) on average. Some sources describe roughly 10 cm as a typical length for the entire wishbone structure. The width (across both bulbs) can be a few inches as well - essentially, the clitoral bulbs curl around the vaginal opening from both sides, almost touching each other under the urethra. Again, individuals can have slightly larger or smaller internal clitorises. These differences generally aren’t noticeable externally, but they might be one reason sensitivity or the way orgasms feel can differ between people.
Sometimes, an especially large clitoris can occur due to hormonal conditions. For instance, exposure to high levels of androgens (male-type hormones) in utero (as in congenital adrenal hyperplasia) can lead to a condition called clitoromegaly, where a baby girl is born with an enlarged clitoris that may resemble a small penis. Certain hormonal disorders or use of anabolic steroids can also enlarge the clitoris in adults. These are medical conditions, however, and not the typical range of variation. In typical anatomy, even a clitoris on the larger end of normal (say a 1 cm glans) is still far smaller than even a flaccid penis.
On the flip side, some have very small clitorises, but as long as the structure is present and sensitive, sexual function isn’t necessarily impaired. It’s worth emphasizing that size doesn’t correlate with sensation - a smaller clitoris can be just as sensitive (or more) than a larger one, since even the smallest clitoris still has thousands of nerve endings.
Finally, the clitoris can be subject to some of the same issues as other body parts. For example, poor hygiene can lead to smegma (a natural buildup of oily secretions) accumulating under the hood, which might cause discomfort if not occasionally cleaned. There are also rare cases of clitoral adhesions, where the hood sticks to the glans (due to scarring or inflammation) and prevents normal movement. Proper gentle cleaning and treating any infections or skin conditions can usually prevent or resolve these issues. Thankfully, serious diseases of the clitoris (like cancer) are extremely rare, though vulvar cancer can in rare instances involve the clitoral area.
In everyday life, most women may not give much thought to the appearance of their clitoris, but understanding that everyone’s is a bit different can be reassuring. There is a wide range of “normal”, and no one should feel self-conscious if their clitoris or vulva doesn’t look exactly like some diagram or image they’ve seen.
Historical Understanding and Cultural Perspectives
Throughout history, the clitoris has had a bit of a tumultuous story - alternating between recognition and obscurity. Ancient anatomists and physicians had some awareness of it, but cultural attitudes toward female sexuality often influenced how (or if) the clitoris was acknowledged in medical texts. Here’s a brief journey through time:
Ancient Knowledge
Some ancient Greek and Roman physicians recognized that female and male genitals were analogous. For example, the philosopher Aristotle and others noted similarities, and there were terms for the clitoris in classical languages (the Greek word kleitoris meaning “little hill”). However, a prevailing idea (not entirely accurate) was that the vagina was essentially an “inverted” penis, and some (like the 2nd-century physician Galen) thought the vagina was the female equivalent of the penis, with the clitoris not given much importance. The clitoris was sometimes conflated with other structures or simply not well-differentiated.
Medieval to Renaissance Discoveries
The Middle Ages didn’t produce much advancement in anatomy, but by the Renaissance period (16th century), anatomists in Europe started to rediscover the clitoris - often claiming to be the first to do so. Historical records show a bit of a “who found it first” controversy. In 1545, anatomist Charles Estienne described the clitoris (from dissections) but mistakenly thought it had a urinary function. A few years later, in 1559, Realdo Colombo published a description of the clitoris as the “seat of women’s delight”, clearly recognizing its role in female pleasure. Colombo even suggested naming it after Venus (the goddess of love) because of its pleasure function. However, another anatomist, Gabriele Falloppio (known for the Fallopian tubes), contested Colombo’s claim, insisting he had found it first (1561) and that others had neglected it. This academic squabble highlights that the clitoris was something of a curiosity - not universally taught, so each “discoverer” thought it novel. Notably, Andreas Vesalius, a famous 16th-century anatomist, doubted these findings and claimed the clitoris didn’t exist in “normal women” - implying it was a rarity or a feature of hermaphrodites. Vesalius’s view shows a stubborn skepticism and perhaps the influence of the era’s discomfort with female sexual anatomy.
Cultural Myths in History
In various historical cultures, there were myths around women with large clitorises. For instance, the term tribade in antiquity referred to a woman (often imagined as a lesbian) who supposedly could use an enlarged clitoris to penetrate others. This was born from the idea that in any penetrative sex, one partner must play the “male/phallic” role - a notion that led to sensational myths about lesbians having big clitorises or needing a phallus. These ideas weren’t based in fact but show how the clitoris was often viewed through a distorted, male-centric lens.
Suppression and “Forgetting”
After the initial flurry of descriptions in the 1500s, you might expect the clitoris to have been a standard part of anatomy. However, its treatment in medical literature remained inconsistent. By the eighteenth and nineteenth centuries, discussions of the clitoris were often muted. In the Victorian era (19th century), a time known for prudish attitudes toward sex, the necessity or importance of female pleasure was downplayed. In fact, there was even a misguided medical practice of clitoridectomy (removal of the clitoris) in some cases - British physician Isaac Baker Brown infamously performed clitoridectomies in the 1860s as a supposed cure for female “hysteria” or masturbation, reflecting deep misunderstandings and control of female sexuality. Going further back, an earlier justification for clitoridectomy came from the 16th-century writings of Jacques Daléchamps, who claimed that many women (particularly in certain regions like Egypt) had overly large, “masculine” clitorises that they used for pleasure, and thus they should be cut off. This horrifying practice and rationale - which today we recognize as female genital mutilation - stemmed from cultural anxieties about women deriving sexual pleasure.
Freud’s Influence
Fast-forward to the early 20th century, and we meet Sigmund Freud. In 1905, Freud proposed the idea that there were two kinds of female orgasm: a “clitoral orgasm” (which he deemed juvenile) and a “vaginal orgasm” (considered the mature, proper form for adult women). He suggested that as girls grow up, they should transfer their sexual focus from the clitoris to the vagina. This theory had no physiological basis, but because Freud was so influential, it cast a long shadow. For decades, the notion that clitoral pleasure was somehow inferior or that a “real” woman orgasmed via intercourse alone made many women feel abnormal if they needed clitoral stimulation. It wasn’t until much later in the 20th century that sex researchers and feminists debunked this idea - notably, in 1970, Anne Koedt wrote “The Myth of the Vaginal Orgasm”, pointing out that the clitoris is the center of female orgasm and criticizing Freud’s assertion as baseless.
20th Century and the Sexual Revolution
In the mid-20th century, researchers like Alfred Kinsey (1940s-50s) and William Masters and Virginia Johnson (1960s) studied human sexual responses. They documented that female orgasm is almost always clitoral in origin, even if achieved during intercourse. Masters and Johnson observed the physiological stages of arousal and noted the clitoris’s role, though interestingly, even their anatomical descriptions were not as complete about the internal clitoris. By the 1970s, as the women’s liberation movement progressed, there was a push to reclaim knowledge of women’s bodies. The book Our Bodies, Ourselves (first published in 1970 by the Boston Women’s Health Book Collective) and feminist health clinics encouraged women to explore their own anatomy, even using mirrors to locate the clitoris and understand their bodies. This helped demystify the clitoris for many and spread awareness that it was normal (and healthy) to enjoy clitoral stimulation.
Modern Rediscovery in Medicine
Shockingly, even by the late 20th century, medical textbooks were still giving the clitoris minimal treatment. Many anatomy books would show the male reproductive anatomy in detail (with the full structure of the penis), but would depict female anatomy with little more than external vulva and internal ovaries/uterus - the full clitoral structure was often missing. This began to change thanks to the work of researchers like Dr. Helen O’Connell, an Australian urologist. In the 1990s, Dr. O’Connell conducted detailed studies of the clitoris using dissections and imaging. In 1998, she published the first comprehensive modern anatomical study of the clitoris. This study (and a follow-up MRI study in 2005) revealed what earlier anatomists had missed or only partially noted: the clitoris is not just a “small nub”, but a substantial organ extending around the vagina, with bulbs that engorge during arousal. O’Connell described the full shape, sometimes likening it to a flower or an orchid - with the external glans as the “bloom” and the internal crura and bulbs as the hidden structure beneath. Her work was revolutionary in the medical community, which had largely ignored this organ.
It turned out that older texts that did mention internal clitoral structures often dismissed them as the “poor homologue” of the penis or a rudimentary organ. O’Connell’s findings firmly established that the clitoris is complex, significant, and anything but “rudimentary”. Since her work, there has been a growing effort to include complete clitoral anatomy in textbooks and medical training, though progress has been slow. As one gynecologist lamented in 2020, references to the clitoris were still scant in medical literature and education: “I read papers all the time, and never do I find mention of the clitoris”, she said. This indicates that while science now knows about the clitoris’s anatomy, the dissemination of that knowledge is still catching up.
In cultural terms, the clitoris has also become something of a symbol of female sexuality and empowerment. Recognizing and valuing the clitoris is tied to acknowledging women’s right to sexual pleasure. In the past, societies that were uncomfortable with women’s sexuality tended to ignore or even physically suppress the clitoris (as with some practices of female genital cutting). Today, educational initiatives aim to spread awareness about the clitoris to ensure women (and their partners) understand it. The more the clitoris is understood, the more myths about female pleasure can be dispelled.
Modern Scientific Discoveries and Ongoing Research
Scientific interest in the clitoris has increased in recent decades, shedding more light on this organ’s anatomy and physiology. We’ve already mentioned Dr. Helen O’Connell’s pioneering work in the 1990s, which was a major milestone. Her detailed dissections and imaging studies (1998, 2005) gave the medical community a much clearer picture of the full clitoral structure. One striking finding was that the volume of erectile tissue in the clitoris is about ten times larger than what had been shown in many anatomical textbooks. This helped correct the misconception that the clitoris was just a “tiny nub”. O’Connell also mapped the nerve pathways of the clitoris, highlighting how nerves branch and supply not only the glans but the entire clitoral complex. This nerve mapping is important, for example, for surgeons - to avoid nerve damage in procedures like pelvic surgeries or in gender affirmation surgeries.
In 2008, French researchers used 3D ultrasound imaging to visualize the clitoris during sexual arousal. The resulting images were the first of their kind, showing how the clitoral bulbs and crura fill with blood and surround the vagina when a woman is aroused. These 3D models confirmed what O’Connell described and helped further educate both medical professionals and the public. The images famously showed the clitoris looking a bit like a flower or a water drop shape around the vaginal canal - which captured public imagination about the “hidden” shape of female arousal.
There has also been research into the number of nerve endings. The oft-cited number of 8,000 nerve fibers in the clitoral glans comes from older histological studies, and some recent work suggests the number could be even higher (possibly up to 10,000). For comparison, the penis glans has around 4,000 nerve endings as a ballpark figure. Knowing this helps explain the sensitivity differences. However, counting nerve endings is tricky, and what matters more is understanding how those nerves contribute to sexual function.
Another area of interest is the role of the clitoris in reproduction beyond pleasure. While not necessary for conception, some scientists have hypothesized that female orgasm (often via clitoral stimulation) might have evolutionary benefits - for instance, the muscle contractions during orgasm could help draw sperm upward (the “upsuck” theory). A recent essay even argued the clitoris has “procreative importance” by encouraging intercourse at optimal times, but this is still a topic of debate. By and large, the consensus remains that the clitoris’s main role is recreational (pleasure) rather than procreative.
On the medical front, awareness of the clitoris is improving treatments and surgeries. For example, surgeons who perform procedures for urinary incontinence or prolapse now take care to avoid damage to the clitoral structures and nerves (earlier techniques sometimes inadvertently reduced clitoral sensation). There are also reconstructive surgeons working on procedures to restore some function to women who have undergone female genital mutilation (FGM) by reconstructing parts of the clitoris - these efforts are informed by the detailed anatomical knowledge brought forth by modern research.
Educational outreach is also a form of “ongoing research” - organizations and sex educators are actively working to spread the updated understanding of clitoral anatomy. This includes incorporating 3D models in teaching, updating medical school curricula, and public health messages that stress the importance of female pleasure for overall sexual health. The hope is that as knowledge becomes widespread, the clitoris will no longer be a mystery organ.
In summary, scientific discoveries in the last few decades have revolutionized our understanding of the clitoris and corrected many errors from the past. We now know the clitoris is a complex organ, much larger than once thought, and crucial to sexual response. Research is continuing, particularly into how clitoral stimulation contributes to various aspects of sexual health, and there’s growing recognition that studying female pleasure is just as important as studying any other aspect of human biology - something that was neglected for far too long.
The Bottom Line
The clitoris is a remarkable organ that epitomizes the phrase “small but mighty”. It may be small in visible size, but it holds immense importance for sexual pleasure. To recap, the clitoris is located at the top of the vulva and consists of an external glans (the sensitive tip) and a larger internal structure (the shaft, crura, and bulbs) made of erectile tissue. Its function is to provide pleasure and help facilitate arousal and orgasm - it’s packed with nerve endings that make it the most sensitive spot on the female body. In terms of structure, it’s often compared to an iceberg: the little bit you see is just a hint of the bigger form beneath the surface. There is a rich history behind our understanding of the clitoris, with periods where it was celebrated and studied, and other times when it was ignored or suppressed due to cultural attitudes. Many myths have surrounded it, but modern knowledge allows us to dispel those and appreciate the facts.
For a general audience, the key takeaway is that the clitoris is central to female sexual experience. Knowing about it - whether for oneself or a partner - can lead to better, more satisfying intimacy. There is nothing taboo or shameful about this body part; it’s simply a part of human anatomy, as deserving of understanding as a heart or a knee (and arguably more fun!). As science and society continue to shed light on the clitoris, it’s becoming more accepted to talk about and include in education. This empowerment through knowledge helps ensure that people with clitorises can fully enjoy their bodies without mystery or stigma.
In short, the clitoris is an amazing organ of pleasure, with an anatomy that is both elegant and purpose-built. By learning about the clitoris - its location, how it looks, how it works, and its history - we foster a healthier, more informed view of female sexuality. And with that understanding, hopefully, comes greater appreciation and respect for the role of pleasure in human life.
Resources
- Wikipedia - Clitoris
- The Guardian - The sole function of the clitoris is female orgasm. Is that why it’s ignored by medical science?
- Cleveland Clinic - Clitoris: Anatomy, Location, Purpose & Conditions
- Vice - The Biggest-Ever Orgasm Study Tells Us More About How Women Come
- Clue - What is the Clitoris?